
- Halitosis prevalence is not uniform worldwide and varies due to differences in culture and perceptions of smell.
- People over 60 years old can have a higher incidence of malodor due to the occurrence of systemic diseases and regular intake of medications.
- Having an objective, quantitative, and precise method for measuring halitosis can help healthcare professionals diagnose and treat its various types.
Halitosis or oral malodor has been a serious problem for thousands of years. Ancient Hebrew texts over two thousand years old indicate that oral malodor in one partner was considered sufficient legal ground for terminating marriages! Writings from early Roman, Greek, Christian, and Islamic societies also have similar references. Nevertheless, scientific study of halitosis began only in the 1940s-1950s. Its prevalence varies across the globe for a variety of reasons, including the lack of a uniform measurement method. This article explores information about the prevalence and causes of halitosis, which can help healthcare professionals share relevant information with patients.
Types of Halitosis
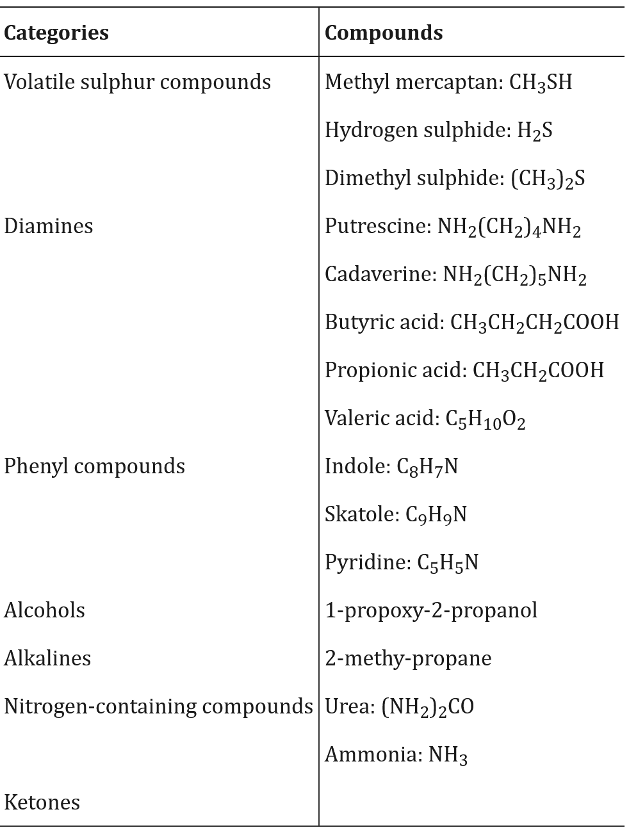
Halitosis is the bad odor from the mouth and cavities of the nose, pharynx, or sinuses. It is also called bad breath, oral malodor, fetor oris, and fetor ex oris. It is the smell caused by volatile molecules, such as sulfur, phenyl, amines, alcohols, aliphatic compounds, short-chain fatty acids, and nitrogen compounds, produced for pathological and non-pathological reasons; see Table 1. The exact chemical involved depends on the cause of halitosis.
Halitosis is the third most common reason for visiting a dentist. Halitosis is categorized into genuine halitosis, pseudo-halitosis, and halitophobia.
- Genuine halitosis: Only genuine halitosis is clinical and can be further subdivided into physiologic halitosis or pathologic halitosis. Pathologic halitosis can be oral and extra-oral.
- Oral: Around 85% of genuine cases are oral and result from periodontitis, poor oral hygiene, or a pathologically coated tongue.
- Non-oral: Up to 10% of malodor comes from the ears, nose, and throat (ENT), of which 3% is from tonsils. Around 5% of non-oral malodors can be due to diseases of other organs, such as the respiratory and gastrointestinal systems, the liver, the kidneys, the endocrine system, hematologic conditions, and metabolic conditions.
In pathological halitosis, bacterial activity in the mouth produces volatile sulfur compounds such as hydrogen sulfide, methyl mercaptan, and dimethyl sulfide. Bacteria can grow in the grooves and fissures on the dorsal side of the tongue.
- Pseudo-halitosis: It is the phenomenon in which people do not have halitosis symptoms but believe they have bad breath. These patients can be treated by dentists.
- Halitophobia: People suffering from halitophobia complain of halitosis even though they have no malodor. When the condition persists after patients have been treated for genuine halitosis or pseudo-halitosis, dentists diagnose halitophobia. People suffering from halitophobia cannot be cured by dentists but must be referred to psychological specialists.
Since treatments differ in each type of halitosis, an accurate diagnosis is crucial. In many cases, patients suffering from halitophobia may not accept help from a psychologist or psychiatrist, as they strongly believe they have malodor. An objective and quantitative means of measuring halitosis is suggested as a way to help and show people with pseudo-halitosis and halitophobia that malodor does not exist.
Table 1. “Volatile molecules contributing to oral malodor,” Bollen and Beikler (2012). (Credits: doi: 10.1038/ijos.2012.39)
Effects of Halitosis
Halitosis is not life-threatening, but it can cause considerable emotional distress, social isolation, health deterioration, and economic stress to sufferers.
- Social problems: People suffering from real or imagined halitosis suffer anxiety and withdraw from social life.
- Dental health deterioration: It may hinder visits to the dentist, worsening real cases of halitosis and other dental problems.
- Emotional distress: Halitosis can cause low self-esteem and self-confidence and affect marriages, quality of life, and career aspirations. It can lead to depression, loneliness, substance abuse, divorce, and suicidal tendencies.
- Economic stress: People can waste many productive hours addressing malodor and spend considerable sums of money on treating the real or perceived problem. For example, Americans spent $700 million dollars on mouthwash in 2000.
Due to its impacts, halitosis is a problem that people and healthcare professionals cannot ignore.
Prevalence
Globally, halitosis affects 22% to 50% of the total population. However, there are differences in the prevalence of the problem across geographic regions, ages, education levels, oral hygiene, systemic diseases, and the lack of uniform evaluation methods. The percentages are higher when self-reported than when halitosis is detected clinically.
Geographical differences
The differences in the geographical prevalence of halitosis may be due to variations in culture, odor perception, and diet.
- In the USA, 50% of the population has halitosis.
- In China, halitosis is found in 6-23% of the people.
- Among Indians, the incidence of halitosis is 21-35%.
- In Sweden, only 4% of a sample group of men and women had halitosis.
- In Brazil, around 15% of university students and their families had halitosis.
- In Japan, 15% had halitosis, and in Tokyo, it was 20%.
- In Kuwait, 25% had bad breath.
- In France, 22% showed halitosis.
Gender
Halitosis is not related to gender. Some studies found that the prevalence of halitosis is higher among men than among women. For example, in Brazil, among adults over 20 years, more men than women had halitosis. In India, the reverse trend was seen, and women had a higher incidence of halitosis; among dental students, 21.7% of men and 35.5% of women had halitosis.
Age
Most studies have shown an increase in malodor with age. For example,
- In Turkey and Switzerland, 28% of people over 60 years old had halitosis.
- In the USA, 43% over 60 years had halitosis.
Oral health, the existence of systemic diseases, the use of medication, and hyposalivation could be some of the reasons that explain the higher incidence of halitosis among senior citizens.
Other Factors
Among other factors that influence the prevalence of halitosis are oral hygiene habits, diet, medication, and lifestyle. Among 1% of people with halitosis, diet and medication were the causal factors.
- Oral hygiene habits: While people report brushing their teeth once a day, only half report brushing twice, which is necessary for oral health. Other hygiene measures, such as mouthwash use, flossing, and tongue cleaning, are less frequent, which can increase the risk of malodor. Mouth breathing also increases malodor. Irregular visits to the dentist and checkups that can identify oral conditions such as periodontitis are other factors.
- Diet: Food high in carbohydrates can increase malodor.
- Lifestyle: Smoking, vaping, and regular medication can increase halitosis.
Higher levels of education were associated with lower self-reports of halitosis, probably because of more awareness of oral health issues, better oral care, and therefore, fewer oral problems.
Diagnosing Halitosis
Diagnosing and treating halitosis can be challenging due to its various origins and causes. There is also an absence of standard guidelines for diagnosis, and methods can vary. One of the simplest yet precise and rapid means of measuring halitosis is the use of Interscan’s Halimeter. It is precise enough to measure odor-forming chemicals in ppb (parts per billion) levels.
The objective, quantitative, and impersonal nature of the instrument can also help healthcare professionals distinguish genuine halitosis from pseudo-halitosis and halitophobia, thereby guiding patients with the latter two conditions to seek appropriate treatments.
Contact us for more information on the Hailmeter for your clinic’s needs.
Sources
Akaji, E. A., Folaranmi, N., & Ashiwaju, O. (2014). Halitosis: a review of the literature on its prevalence, impact and control. Oral Health Prev Dent, 12(4), 297-304.
Al Rubaye, S. F., kadhim Alkhazaali, N. B., & Motea, Y. H. (2026). Oral hygiene habits, dental conditions, and self-perceived halitosis across age groups: A cross-sectional survey. Adolescência e Saúde, 21(1), 13-22.
Aylıkcı, B. U., & Colak, H. (2013). Halitosis: From diagnosis to management. Journal of natural science, biology, and medicine, 4(1), 14–23. https://doi.org/10.4103/0976-9668.107255
Bollen, C., Beikler, T. Halitosis: the multidisciplinary approach. Int J Oral Sci 4, 55–63 (2012). https://doi.org/10.1038/ijos.2012.39
Dudzik, A., & Chomyszyn-Gajewska, M. (2014). Pseudohalitoza i halitofobia [Pseudohalitosis and halitophobia]. Przeglad lekarski, 71(5), 274–276.
Kapoor, U., Sharma, G., Juneja, M., & Nagpal, A. (2016). Halitosis: Current concepts on etiology, diagnosis and management. European journal of dentistry, 10(2), 292–300. https://doi.org/10.4103/1305-7456.178294
Moreno, L. B., Colussi, P. R. G., Marostega, M. G., Rosalen, N. P., Rösing, C. K., & Muniz, F. W. M. G. (2022). Self-reported halitosis and associated factors among older adults: A cross-sectional study. Journal of Oral Biology and Craniofacial Research, 12(4), 431-436.
Murata, T., Yamaga, T., Iida, T., Miyazaki, H., & Yaegaki, K. (2002). Classification and examination of halitosis. International Dental Journal, 52 Suppl 3, 181–186. https://doi.org/10.1002/j.1875-595x.2002.tb00921.x
Sanz M, Roldan S, & Herrera D. (2001). Fundamentals of breath malodour. J Contemp Dent Pract 2:1–17.
Setty, S. Solution for halitophobics. Br Dent J 195, 64 (2003). https://doi.org/10.1038/sj.bdj.4810368
Söder, B., Johansson, B., & Söder, P. O. (2000). The relation between foetor ex ore, oral hygiene and periodontal disease. Swedish Dental Journal, 24(3), 73-82.
Wu, Z., Tan, W., Wang, T., Ke, T., & Liu, F. (2025). Trends and hotspots in global halitosis research: A bibliometric analysis from 2010 to 2025. Medicine, 104(52), e46830. https://doi.org/10.1097/MD.0000000000046830
Yaegaki, K., & Coil, J. M. (2000). Genuine halitosis, pseudo-halitosis, and halitophobia: classification, diagnosis, and treatment. Compendium of continuing education in dentistry (Jamesburg, N.J. : 1995), 21(10A), 880–890.